
A piece about scientific aspects of depression and the likes. I got asked to do a piece about the advances in the psycho-pharmaceutical field but I fear I could not find an awful lot in that area. To give a bit more information about the issue I decided to add a few pieces about what depression is and two big drugs that being used to combat the symptoms.
To start off we should know what a depression is biologically, if we would know this exactly we could produce very specific medicine. What exactly happens to the body in a depression is not known, however there are two leading theories. The monoamine theory and the diathesis-stress model.
Monoamine theory
Clinical depression results from low levels of serotonin and norepinephrine (=neurotransmitters) in the brain. The monoamine oxidase inhibitors, tricyclic antidepressants and selective serotonin reuptake inhibitor are antagonists of serotonin en norepinephrine. Because these antidepressants reduce the symptoms of patients it would mean that serotonin and norepinephrine are indeed the problem in people who suffer from depression et cetera. Genetically this would mean that people with a depression have a monoamine deficiency. However there are also some cases in which the antidepressants do not work, indicating that this theory is not complete or correct.
The other model is the diathesis-stress model of depression
This theory suggests that people inherit a genetic disposition to depression. This genetic ‘trait’ is not capable of triggering a depression on its own but it is triggered by a certain stressful moment in life.
This theory is sustained because people with depression produce more of a specific kind of hormones than people without a depression. Specifically; corticotrophin releasing hormone, glucocorticoids and adrenocorticotropic hormone.
When injected with lexamethazone people without depression reduce the release of glucocorticoids. (This is done by a cellular process called suppressing which I will not go into deeper.) People who suffer from depressions do not reduce the release of this hormone, suggesting a genetic problem with the parts of DNA regulating the expression of these hormones.
But how do we battle these problems? What kind of medicine exist?
As there are many medicines that can be prescribed, I shall only write a piece about the two most important ones, lithium and SMRI’s.
How does lithium work? How was it discovered?
John Cade, an Australian psychiatric mixed the urine of manic patients with lithium and he noticed that it formed soluble salts. He injected lithium into guinea pigs to see if he could induce mania in the animals. Instead of the mania, they became very very calm. He concluded the animals were calmed by the lithium and it was not the fault of ureic acid.
We know now that John Cade’s conclusion was a bit silly to make. The doses he used with the guinea pigs did not induce calmness, but the guinea pigs were made extremely nauseous. He mistook the sickly guinea pigs for calm guinea pigs. When we treated people who suffered from manic depsression with lithium however, it did seem to work and reduce their symptoms. Only in the right dosages though.
Later in the 60’s it was discovered that it not only reduced mania, it was also reducing the symptoms of depression. It was used as a mood stabilizer but it is nowadays mostly supplanted by other compounds. How it exactly acts in the body as an element, is of yet unknown. We just know that it works and what dosages to use.
SMRI’s
Another important compound is “Selective monoamine-reuptake inhibitors”. These compounds are also known as fluoxetine. An example of these SMRI’s is Prozac, the first SMRI that was developed for commercial use.
But why is this drug so immensely popular? This is due to the fact that the drug has relatively few side effects and can be used for hundreds of mental issues including, lack of self-esteem, fear of failure, excessive insensitivity for criticism and the inability to feel pleasure.
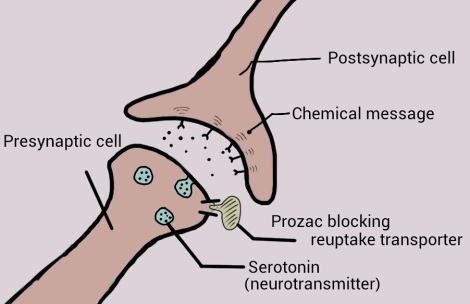
The synapses of neuron cells. Black dots indicate serotonin. (Blue blob is a capsule and black ‘forks’ are the serotonin-receptors).
The synapses of neuron cells, where the serotonin neurotransmitter gets sent from one cells to another. Prozac is blocking the re-uptake of the neurotransmitter resulting in a higher concentration of serotonin between the cells. The lack of that serotonin between the ends is what is believe to be a cause of depression.
Advancements in the field of psycho-pharmaceuticals
One of the big breakthroughs lately is the way people take up the medication. Pills are very clumsy and take a while to get absorbed by the body.
As people with bipolar disease and schizophrenia have symptoms which include irritability, tension and hostility, a new drug delivery system has been produced. This system focuses on the fast treatment of the symptoms. It is a new fast system to inhale laxapine to reduce the more hostile symptoms that people experience from or during a mood change.
Although there are many drugs still being tested, lithium is still one very important drug in this field of work. It is still the benchmark comparator agent for all the new drugs that tackle symptoms of depression, schizophrenia and bipolar disease.
Nowadays not much research is being done about new drugs more and more of the drugs that were originally produced for schizophrenia and epilepsy are being used for the treatment of bipolar disease or depression. However the most progress in dealing with the symptoms is being made outside the pharmaceutical field, as the roles of RCT’s, psychological intervention, psychotherapies, cognitive behavioral therapy and psycho-educational approaches are becoming of greater importance. Therapy is starting to play a larger role than the medication.
Due to the lack of knowledge of what exactly goes on in the body on molecular level the process in the advancement of psycho-pharmaceuticals in not optimal. The advances in the field of genetics are the most of use for psycho-pharmaceuticals. The advances that will be made in this field can be used to get a better understanding about what exactly we are treating and use this knowledge to make a more targeted solution for the symptoms at hand. In short, the better we know what we’re dealing with, the better we can treat it.
As of yet the details and specifics of the molecular changes in people with bi-polar disease, depression, schizophrenia and other mental issues are very sketchy. To really get a revolution and new innovations in this field is to get more fundamental research done on the subject of the disease itself rather than the treatment of it. Until then, it’s a steady although rather slow progress.
References;
Major advances in bipolar disorder – P. Mitchell et al. Aug 2004 207-210 The Medical Journal of Australia.
John P. J. Pinel – Biopsychology 6th edition
Medical News Today – Joseph Nordqvist
Advancements in the psycho-pharmaceutical department.
From December 27 ADUSAVE (Laxapine).

Where can I find a “neutral” psycho-pharmacologist that will help me evaluate which drugs can be eliminated from my regimen. As background, 30 years ago I suffered a severe concussion in an auto accident. Within the following six months I developed severe depression and related symptoms. My psychiatrist tried one on one therapy which led to no discovery. He then introduced me to imipramine and within three weeks I was back in control of life, regained my interest in hobbies and activities and was able to re-focus on my job. This went on for about 10 years, or until the advent of SSRI’s (zoloft}. Following open heartsurgury I became “foggy”, confused, unable to focus and depressed and the doctor introduced wellbutrin as well the problem was rectified and I continued working. Then, 3 years later, after a bout with cancer, the radiation seemed to give me “chemobrain” and many of the “foggy”, memory, focus, etc. problems returned.
In an effort to sharpen “executive skills” (I was in a very high profile, demanding job) we ended up on the following: wellbutrin xl 300mg,
pristiq 100mg, and lamotrogine 300mg as my “brain drugs” and 200 mg provigil. In addition, I take celebrex, a small amount of metropolol trartrate, lipitor and plavex.
Just to make the mix complete I have had 3 neck surgeries and one for a broken shoulder – all in the last year and have just now started to reduce oxycontin from 30mg three times per day – now 20 mg 3 times per day – soon to be 10 mg 3 times per day etc. Also, for flare-up pain I take Norco when needed – maybe once a day.
I am looking for a medical professional who will help me evaluate which drugs to eliminate and how to do so safely. The pain medications are already being scheduled to be discontinued, but I have a feeling that the “brain” drugs could use some correction. Do you know of anyone or group of people that could advise me.
Thank you,
Peter Nestler
Hello,
I’m afraid that the best information you could get on that subject is at your local hospital or your general practitioner. I couldn’t really give an educated answer on those kind of subjects I’m afraid (sorry!) Perhaps visit another psychiatrist? Above all else I wish you the very best on your recoveries though,
Good luck and get well.